Microscopic polyangiitis (MPA) is part of the anti-neutrophil cytoplasmic antibodies (ANCA)-related vasculitis, which usually presents as renal pulmonary syndrome. It is defined as a pauci-immune necrotizing small vessel vasculitis, which usually affects the kidneys, followed by the lungs. It also presents systemic symptoms. The etiology of MPA is still unclear, but evidence reinforces the autoimmune mechanisms as the main etiopathogenic factor. Aortic valve stenosis (AS) is not an uncommon disease whose etiology varies according to geographical differences and the patient’s age. The
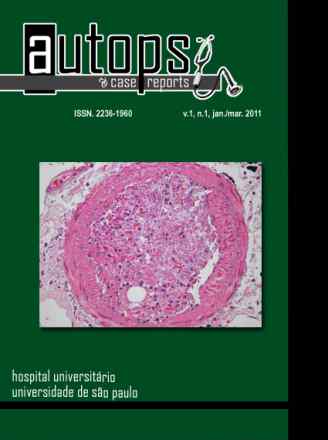
natural history of AS begins with a prolonged asymptomatic period, but when symptomatic, respiratory failure is one of its main clinical presentations. The authors present the case of a 55-year-old woman who was admitted with the diagnosis of renal failure, anemia, and a cardiac murmur. The patient had been recently diagnosed with pneumonia. During hospitalization, diagnostic workup disclosed a normal kidney size as well as parenchymal thickness. A renal biopsy was undertaken but the specimen was exiguous, showing 4 sclerotic glomeruli and 1 glomerulus with crescentic glomerulonephritis. The search for ANCA was positive. The investigation of the cardiac murmur disclosed AS. The patient, on hemodialysis, presented episodes of respiratory failure, which was interpreted as acute pulmonary edema, but a suspicion of ANCA-related pulmonary renal syndrome was raised. However, the aortic valve replacement was prioritized. While awaiting cardiac surgery, the patient died because of respiratory insufficiency. Autopsy findings concluded that MPA with pulmonary hemorrhage due to vasculitis was the immediate cause of death. Although AS was present at autopsy and classified as moderate/severe, this lesion was a bystander in the process of this patient’s end of life, demonstrating the value of autopsy for medical learning and reasoning purposes.