Strongyloides stercoralis hyperinfection syndrome is classically associated
with impaired host response and implies in an overburden of larvae in its usual
cycle. It has been recognized as a severe and potentially fatal condition in
immunocompromised individuals, especially those using oral corticosteroids.
Infection with Schistosoma mansoni not only increases the susceptibility to
HIV infection, but also promotes progression to disease. The association of
the most severe forms of strongyloidiasis and AIDS is scarcely described, even
more when S. mansoni is also associated. The authors describe a case of a
34-year-old previously healthy male, admitted to the emergency department
with a history of hematemesis associated with dyspnea, hemoptysis, and
fever. He referred homosexual relations for 6 years. Physical examination
showed an ill-looking patient, and was remarkable for tachycardia, tachypnea,
diaphoresis, and pulse oximetry of 70% in room air. Lungs examination
revealed the presence of rales in the left base. Chest radiography showed
a diffuse and bilateral reticulo-nodular pattern. HIV serology was positive.
Empirical antimicrobial therapy and corticosteroids were initiated. On the third
day of hospitalization, petechiae appeared over the periumbilical area, but no
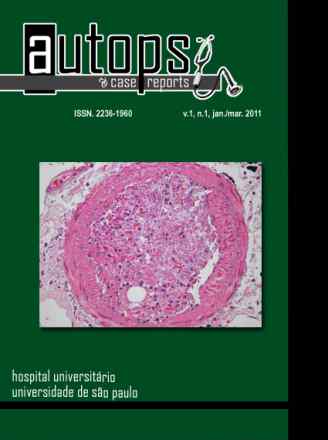
further investigation was undertaken because the patient died soon after. The
autopsy findings were compatible with S. stercoralis disseminated infection,
a hepatic intestinal chronic form of schistosomiasis, and septic shock as the
primary cause of death. The authors call attention to this infrequent association.